Hormones — such as oestrogen, testosterone, adrenaline and insulin — are extremely important chemical messengers that affect many aspects of your overall health. Hormones are secreted by various glands and organs, including your thyroid, adrenals, pituitary, ovaries, testicles and pancreas. The entire endocrine system works together to control the level of hormones circulating throughout your body, and if one or more is even slightly imbalanced, it can cause widespread, major health problems.
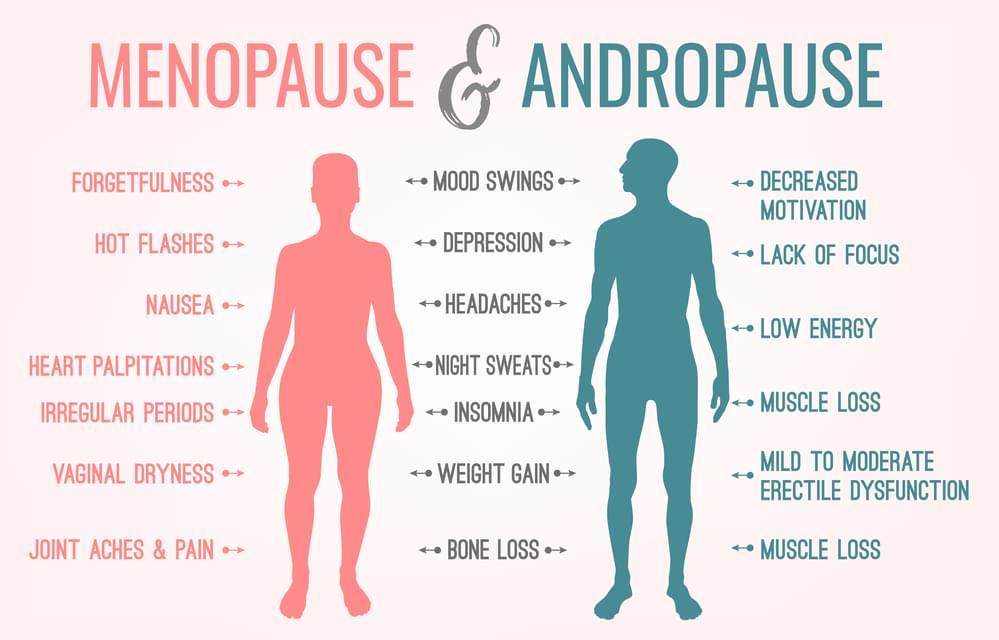
Women in particular are very aware of hormonal changes with each menstrual cycle, which may be accompanied by unwanted symptoms. Later on in life women become acutely aware of the symptoms that accompany pre, peri and menopause. Men too can experience hormonal changes particularly if they are experiencing stress, infertility or problems associated with low testosterone
One of the most frequent questions I am asked in clinic is whether taking HRT will help with menopausal symptoms. This is a complex question as I would firstly examine the symptoms and assess, if indeed they are hormone related, but even better is to find out what is going in the body to assess hormone both from a DNA perspective or how hormones are made and then metabolised in the body. There may be a case for using HRT but there may also be case for being cautious. And whilst some problems can be unbearable, such as hot flushes, there are others that may have a different underlying cause triggering unwanted symptoms, with stress being the most obvious for both men and women.
So What Can we Look At:
PCOS – Polycystic Ovarian Syndrome – It is important to see if you’re pushing your testosterone down a pathway which creates more DHT. You will know this is happening if you have excessive facial hair, weight gain and menstrual irregularities. Sadly this condition is often not diagnosed for some time by doctors, but can lead to infertility, blood test will not reveal this. Which is one good reason for doing the DUTCH test.
PMS – Get to the root cause of your monthly pain and mood swings by evaluating the levels of oestrogen to progesterone and each of their metabolites.
Acne – Acne is a symptom of excessive production of androgen hormones. With women, you’ll see acne on the face, neck, forehead and in some cases the chest and upper arms. The DUTCH test can reveal the androgenic by-products of DHEA and Testosterone so you can find out the true cause of this condition.
Breast Cancer – Some women break down their oestrogen into the metabolite 4-OH-E1 (4 Hydroxy Estrone), which is harmful and may damage DNA and promote tumour development. Find out what your levels are relative to other protective oestrogens such as 2-OH-E1. The ratio of these oestrogen metabolites can be manipulated with certain supplements. However, if you are breaking down your oestrogens well to be excreted, there will be potential risk which comes back to the question of whether HRT is suitable.
HRT Monitoring – If you’re taking hormones, the DUTCH test will show you ranges based upon whether or not you’re pre, peri or post-menopausal. While serum blood tests are just fine, they only offer a superficial picture of hormone levels. The way they break down in your body matters more (urine evaluates this) than the total levels (serum).
Chronic Fatigue – Cortisol testing for metabolites will help you understand why you feel this way and how your adrenals are functioning.
Anxiety – The DUTCH Complete test evaluates cortisol and cortisone which is inactive. Cortisol is a stress hormone. Adrenaline metabolites are evaluated also. If either of these are high or (out of balance) you will feel anxious.
Sleep problems? The Dutch test will evaluate several markers such as melatonin production, free cortisol values, plus your VMA level which is a neurotransmitter metabolite of noradrenaline, which is high in people who are in sympathetic overdrive (which leads to persistent insomnia).
We can also look at how hormones are made and metabolised with a DNA test which is often recommended with the DUTCH test. The Hormones DNA test analyses genes involved in the regulation, synthesis, signalling, transport and metabolism of corticosteroids and sex steroid hormones. It looks at how gene variants affect hormones imbalance and details the nutrients and environmental factors that can influence and improve their balance. The Hormones report is recommended for men and women with hormone imbalance symptoms such as the ones listed above.
Summary
- Hormonal imbalances affect many millions of people worldwide in the form of common disorders, like diabetes, thyroid disorders, menstrual irregularities, infertility, low testosterone and oestrogen dominance
- Symptoms include feeling anxious, tired, irritable, gaining or losing weight, not sleeping well, and noticing changes in your sex drive, focus and appetite
- Causes for hormonal imbalances include poor gut health, inflammation, high amounts of stress, genetic susceptibility and toxicity
- Here’s how to balance hormones naturally: eat an anti-inflammatory diet; consume omega-3s, adaptogen herbal supplements, mushrooms, probiotics and other supplements like vitamin D; get good sleep; exercise; and control stress.
References
- Meilahn, E.N. et al. (1998) ‘Do urinary oestrogen metabolites predict breast cancer? Guernsey III cohort follow-up’. British Journal of Cancer.;78(9):1250-1255.
- Samavat, H. and Kurzer, M.S. (2015) ‘Estrogen metabolism and breast cancer’. Cancer Letters. 356(2 Pt A):231-243.
- Lord, R. S. et al. (2002), Estrogen metabolism and the diet-cancer connection: rationale for assessing the ratio of urinary hydroxylated estrogen metabolites. Alternative Medicine Review.;7(2):112-129.
- Woods, N.F. et al. (2009) ‘Cortisol levels during the menopausal transition and early postmenopause: observations from the Seattle Midlife Women’s Health Study’. Menopause; 16(4):708-718.
- Woods, N.F. et al. (2006) ‘Increased urinary cortisol levels during the menopause transition’. Menopause.13(2):212-221.
- Colditz, g, Hankinson S, et al (1995) The use of estrogens and progestins and the risk of breast cancer in postmenopausal women. The New England Journal of Medicine, 332 (24)